Journal Information
Article Information
성인 클라이언트의 참여 향상을 위한 작업치료 중재의 효과: 체계적 고찰
Author Information
Objective:
The purpose of this study was to examine the trend of interventions improving participation of occupational therapies’ clients and to provide evidence and implications regarding occupational therapy practice for client participation.
Methods:
For the main keywords of a database search, “Participation AND Occupational therapy AND Intervention” were used. Using Scopus, PubMed, and Google Scholar, we systematically examined papers published in journals from January 2005 to April 2015. A total of 12 studies were included in the analysis.
Results:
The results revealed the level of quality and trend of each study, the types of intervention, the environments provided during the intervention, the diseases of the participants, the applied tools, and dependent variables measured through participation. The quality and quantity of the studies were shown to be improving. In addition, the interventions were mostly provided for chronic conditions in the form of a self-management program in a community setting. The tools were used by the researchers following their research intention. Quality of Life (QoL) through participation was the most frequently measured condition.
Conclusion:
Through this systematic review, we were able to determine and understand the trends in occupational therapy service for improving participation. In the future, based on this study, research on intervention for improving participation may be further developed.
목적 :
본 연구에서는 참여 향상을 위한 중재를 방법과 내용을 분석하여 작업치료 임상현장에 적용할 수 있 는 근거를 정립하는 것을 목적으로 실시하였다.
연구방법 :
전자 데이터 베이스인 Scopus, Pubmed와 Google scholar를 사용하여 2005년부터 2015년까지 의 논문을 검색하였다. 주요검색 용어로 “Participation AND Occupation therapy AND Intervention”을 사용하였다. 2차 분류를 통하여 최종적으로 12개의 연구를 분석대상으로 선정하였다.
결과 :
결과는 연구의 질적 수준 및 동향, 중재 방법의 종류, 중재가 적용된 환경, 중재의 대상 클라이언트, 참여 평가도구, 동시에 측정된 종속변인을 중심으로 정리하였다. 연구의 질적 수준과 논문의 편수는 증 가하고 있는 양상이며, 중재는 만성질환 환자를 중심으로 지역사회 내에서의 자기관리 프로그램을 가장 많이 시행하였다. 평가도구는 연구자의 연구 의도에 따라 다양하게 사용하는 양상을 보였으며, 연구자들 은 ‘삶의 질’을 참여와 동시에 가장 많이 측정하였다.
결론 :
이번 연구를 통하여 참여 향상을 위한 작업치료 서비스에 대하여 이해하고 그 현황을 종합적으로 알 아봄으로써 임상적 근거를 제공하고자 하였다. 추후에는 본 연구 결과를 바탕으로 참여 증진을 위한 작 업치료 서비스에 대한 연구가 더욱 활발하게 이루어져야 할 것이다.
Ⅰ서 론
국제 기능 장애 건강 분류(International Classification of Functioning, Disability and Health; ICF)는 세계보건 기구(World Health Organization; WHO)로부터 2001 년에 발표된 이후 건강 및 장애와 관련한 틀을 제공하고 표준화된 용어를 제정함으로써 건강 및 보건 관련 분야 전문가들의 의사소통을 원활하게 하고있다([Üstün, Chatterji, Bickenbach, Kostanjsek, & Schneider, 2003]). 분류 체계를 보면 크게 두 부분으로 나누어져 기능(functioning) 과 장애(disability)를 다루며 문맥적 요소(contextual factors)를 포괄한다. 기능과 장애는 다시 신체 기능 및 구조(body functions/body structures), 활동(activities), 참여(participation)의 세 가지 하위 구성요소로 나누어진다.
ICF에서는 이 세 가지의 하위 구성요소 중 ‘참여’를 ‘삶의 상황에 대한 개입(involvement)’이라고 정의하고 있는데, 이는 사회적 건강(social health)과 기능 (functioning)을 중립적으로 나타내는 표현으로 사용된 다([Magasi & Post, 2010]). ICF가 발간되기 전에는 참 여에 대한 전문가들의 정의가 일치하지 않는 경향이 있 었다([Locke & Schweiger, 1979]; [Vroom & Jago, 1988]). 하지만 2014년 발행된 작업치료 실행체계 3판 (Occupational Therpay Paractice Framework: Domain and Process-3rd edition; OTPF-3)에서 ICF에서 제시한 참여의 정의를 따르고 있으며, 최근 간 호학에서도 전문가들과의 효과적인 의사소통을 위하여 이러한 정의를 따를 것을 지향하고 있는 등([Kearney & Pryor, 2004]) ICF의 정의를 중심으로 타 전문가 및 작 업치료 안에서도 참여의 정의에 대한 일치점이 생겨나고 있다.
작업치료 서비스의 대상이 되는 여러 질환군의 클라이 언트는 질병의 특징에 따라 참여의 제한을 겪게 된다. 뇌 졸중 환자의 이동능력 제한, 우울감, 인지적 손상, 피로, 사회적 관계, 활동의 개입(engagement)에 대한 자기효 능감의 부족은 모두 참여 제한으로 이어진다([Chau, Thompson, Twinn, Chang, & Woo, 2009]; [Kubina, Dubouloz, Davis, Kessler, & Egan, 2013]; [Mayo, Bronstein, Scott, Finch, & Miller, 2014]). 또한 외상성 뇌손상 (Traumtic Brain Injury; TBI) 환자의 경우 기 억력, 집중력, 실행 능력의 감소로 약먹기, 일정 관리하 기, 약속 지키기 등과 같은 일상의 활동에 참여하는 것에 어려움을 보인다([Cifu et al., 1997]; [Conboy, Barth, & Boll, 1986]). 이외에도 다발성 경화증(Multiple Sclerosis; MS) 환자들은 피로로 인한 일상적 활동 참여 의 손상을, 저시력 노인들은 사람들의 얼굴과 표정을 알 아보기, 휴대폰 사용하기 등 사회적 과제 참여의 제한이 있다([Chaudhuri & Behan, 2004]; [Tejeria, Harper, Artes, & Dickinson, 2002]; [West et al., 1997]). 이러한 참여의 제한은 클라이언트의 삶에 있어 중요한 영향을 끼친다. 실제로 지역사회에 거주하는 만성 뇌졸중 환자 에게 있어 활동과 참여 제한은 낮은 삶의 만족도와 삶의 질 저하에 영향을 미치는 것으로 밝혀졌다([Hartmanaeir, Soroker, Ring, Avni, & Katz, 2007]; [Mayo, Wood-Dauphinee, Cote, Durcan, & Carlton, 2002]). 일반인을 대상으로 한 연구에서는 활동 참여의 동기나 높고, 실제로 많은 활동에의 참여를 보이는 사람이 낮은 동기와 참여를 보이는 사람보다 삶의 질이 높다는 결과 가 보고되었다([Huang, Lee, & Chang, 2007]).
참여의 정의 및 개념정립이 확실해지기 시작하고 사람 들의 관심이 늘어나면서, [Dahl (2002)]은 재활의 목적이 참 여의 증진으로 이어질 것이라고 제언하였다. [Christiansen, Baum과 Bass-Haugen (2005)]은 작업치료사들이 ICF 에 기초한 ‘참여’에 집중해야 한다고 보고하였고, [Hildebrand, Brewer과 Wolf (2012)] 역시 최근 재활의 목적이 참여의 증진을 많이 포함하고 있다고 보고하였다. [Wolf, Chuh, Floyd, Mclnnis와 Williams (2015)]는 뇌 졸중 후 사회 참여와 작업영역의 향상을 위한 작업기반 중재를 근거기반 고찰을 통하여 제시하면서, 작업기반 중재가 뇌졸중 후에 사회 참여의 향상을 가져온다는 임 상적 의의를 보고하였다. 또한 [Berger, McAteer, Schreier와 Kaldenberg (2013)]는 저시력 노인들의 여 가와 사회 참여를 향상시키는 중재에 대한 체계적 고찰 을 통하여 문제해결적 접근이 여가 및 사회 참여를 향상 시키는 데에 가장 강력한 근거가 있다는 것을 확인하였 다. [Yu와 Mathiowetz (2014)] 역시 다발성 경화증 환자 에 대한 체계적 고찰을 통하여 사회 참여 향상을 위한 근 거를 제시하였다.
또한 참여의 제한을 객관적으로 측정하려는 요구가 증 가되면서 참여에 대한 평가도구가 증가하게 되었다. [Perenboom과 Chorus (2003)]와 [Magasi와 Post (2010)]는 고찰 연구를 통하여 ICF에 따른 참여 평가도 구를 제시하였다. 두 연구 모두 ICF의 활동과 참여 부분 에서 총 9가지의 영역(Learning & Applying Knowledge, General Tasks & Demands, Communication, Mobility, Self-Care, Domestic Life, Social Interactions, Major Life Domains, Community, Social, & Civic)로 부터 세분화된 ICF 코드에 따라 제시된 평가도구들을 분 석하였다. [Perenboom과 Chorus가 2003]년에 제시한 평가도구들 중에서는 9가지 카테고리를 모두 포함하는 평가도구가 존재하지 않은 반면, [Magasi와 Post가 2010] 년에 제시한 평가도구들 중 두 가지는 총 9가지의 카테고 리를 모두 포함하고 있었다. 이는 시간이 지남에 따라 참 여에 대한 개념이 확고해지고 그에 따른 평가도구 역시 체계적으로 개발되고 확립되어지고 있음을 시사한다.
이렇듯 참여에 대한 개념이 확립되어감에 따라서 작업 치료 분야에서 참여의 증진을 위해 어떠한 서비스를 제 공하는지에 그 근거를 제공하는 것은 중요하다. 하지만 아직까지 참여를 주제로 한 작업치료 관련 고찰 연구를 확인해보면 특정 진단군과 중재 방법에 대한 고찰 연구 가 진행되어 있을 뿐, 참여 증진을 위한 다양한 중재가 어떤 진단군에서 어떤 형태로 제공되고 있는지 종합적으 로 정리되어 있지 않으며, 그 중재의 효과를 확인하기 위 해서 어떤 평가도구가 사용되고 있는지 한눈에 확인하기 힘들다([Berger et al., 2013]; [Wolf et al., 2015]; [Yu & Mathiowetz, 2014]). 또한 중재의 효과가 아닌 참여를 측정하는 평가도구의 비교 및 특정 진단군의 참여 수준 에 대한 연구가 다수 진행되어 왔다([Lund, Nordlund, Bernspång, & Lexell, 2007]; [Lundström, Lilja, Gray, & Isaksson, 2015]; [Noonan, Kopec, Noreau, Singer, & Dvorak, 2009]; [Magasi & Post; 2010]; [Perenboom & Chorus, 2003]).
따라서 본 연구에서는 참여를 증진시키기 위한 중재가 어떠한 진단군에, 어떠한 형태로 제공되고 있는지 알아보 고, 관련된 정보를 종합적으로 정리하여 제시하고자 한다.
Ⅱ연구 방법
1.검색 방법 및 분석 대상
2005년 1월부터 2015년 7월까지 해외학회지에 게재 된 논문을 Scopus, PubMed와 Google scholar를 통하 여 검색하였다. 주요 검색용어는 “Participation AND Occupational therapy AND Intervention”을 사용하였 다. 각 데이터베이스에서 검색된 총 718개의 문헌 중 영 어로 쓰여 지지 않은 논문, 대상자가 18세 이하 아동·청 소년인 논문, 데이터베이스 간 중복된 논문, 초록에 ‘participation’과 ‘intervention’이 동시에 포함되지 않 은 논문은 제외하였다. 그 결과 1차적으로 총 48개의 논 문이 선정되었다. 이후 아래의 배제기준에 따른 분석을 통하여 최종적으로 12개의 논문을 본 연구에 분석 대상 으로 사용하였다. 높은 근거 수준을 제시하기 위하여 근 거를 기반으로 한 연구의 질적 수준 분석 모델([Arbesman, Scheer, & Lieberman, 2008]) 중 Level 1, 2, 3에 해당 되는 경우의 논문만을 분석하였으며 이에 따라 Level 4, 5에 해당하는 개별실험 연구 및 사례연구는 제외되었다. 분석은 제1저자와 2저자가 진행하였다(Figure 1). 국내 학회지에 게재된 논문의 경우 RISS, KISS, 국립중앙도 서관을 통하여 “작업치료 AND 참여 AND 중재” 등의 용 어를 통하여 검색한 결과 총 55개의 문헌이 검색되었 으나 55개의 문헌은 모두 배제기준에 포함되어 제외하 였다.
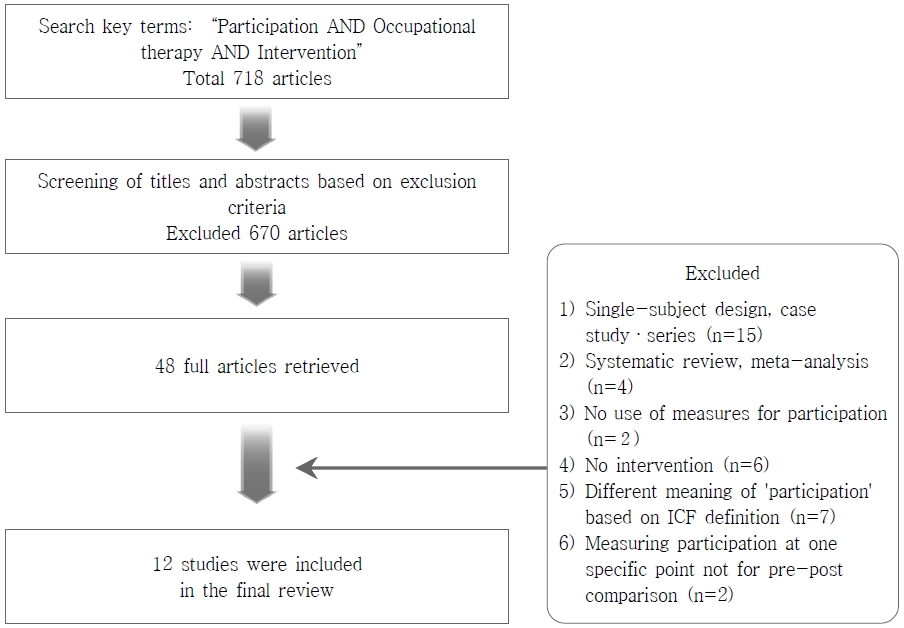 Figure 1.Search Process
Figure 1.Search Process
1)배제기준
(1)
개별실험연구(single-subject designs) 및 사 례연구(case study, case series)인 것
(2)고찰논문(systematic review, meta-analysis) 인 것
(3)참여를 측정하기 위해 평가도구를 사용하지 않은 것
(4)작업치료가 포함된 중재가 독립변인이 아닌 것 (e.g., 조사연구, 작업치료를 제외한 중재가 독립 변인인 경우 등)
(5)참여의 용어가 ICF의 정의를 따르지 않고 다른 의 미로 사용된 것 (e.g., 중재의 참여도, 삶의 질로 사용한 경우 등)
(6)중재를 통한 변화를 확인하기 위하여 중재 전, 후 로 참여를 평가하지 않고 한 시점에서만 단면적으 로 참여를 평가한 것
2.분석 대상 연구의 질적 수준
본 연구에 사용된 논문의 질적 수준을 평가하기 위해 근거를 기반으로 한 연구의 질적 수준(hierarchy of levels of evidence for evidence-based practice) 분석 모델을 사용하였다. 이 분류기준은 [Arbesman 등(2008)] 에 의해 개발된 것으로, 연구의 질적 수준을 평가하기 위해 널리 사용된다. 체계적 고찰, 메타분석, 무작위 대조연구는 Level 1로 가장 상위에 있으며 두 집단 비무작위 연구는 Level 2, 단일 집단 비무작위 연구는 Level 3, 개별실험연 구와 조사연구는 Levle 2, 사례연구는 Level 5로 Level의 단위가 높아질수록 근거 수준은 낮아진다.
Ⅲ연구 결과
1.분석 대상 연구의 질적 수준 및 동향
분석 대상 논문 총 12편의 질적 수준을 분석한 결과, 가장 높은 수준인 Ⅰ 단계에 해당하는 논문이 7편으로 전체의 58.3%였으며, Ⅲ 단계 수준이 5편으로 전체의 41.7%를 차지하였다(Table 1). 수준에서 7편은 모두 무작위 실험-대조군 논문(Randomized Controlled Trial; RCT)이었다. 또한, 총 검색 년도를 반분하여 년도 별 질적 수준의 변화를 살펴보았을 때 2005~2010년도 사이에 나온 Ⅰ 단계 논문은 2편, Ⅲ 단계 논문은 3편으 로 RCT보다 단일집단 사전-사후 설계 논문이 많았다. 반면, 2011~2015년도 사이에 나온 Ⅰ 단계 논문은 5편, Ⅲ 단계 논문은 2편으로 RCT가 단일집단 사전-사후 설 계 논문보다 많았다. 또한, 논문의 편수 역시 증가하는 경향을 보였다(Figure 2).
| Evidence level | Definition | Frequency |
|---|---|---|
| I | Systematic reviews | 7 (58.3) |
| Meta-analyses | ||
| Randomized controlled trials | ||
| II | Two groups non-randomized studies | 0 (0.0) |
| III | One group non-randomized studies | 5 (41.7) |
| IV | Single subject designs | 0 (0.0) |
| Surveys | ||
| V | Case reports | 0 (0.0) |
| Narrative literature reviews | ||
| Qualitative researches | ||
| Total | 12(100.0) |
 Figure 2.Trend in Level of Evidence of Intervention for Participation
Figure 2.Trend in Level of Evidence of Intervention for Participation
2.참여 향상을 위한 작업치료 중재
1)중재 방법의 종류
클라이언트의 참여 증진을 위한 중재 방법을 논문에서 제시한 용어에 따라 크게 다섯 가지로 분류해 제시하 였다. 그 중 자기관리 프로그램(self-management program)은 6편으로 50.0% 차지하였다. 클라이언트 중심 접근(client-centered approach)과 운동 프로그 램(exercise program)은 각각 2편으로 16.7%에 해당 하였으며, 디지털 기기를 이용한 중재와 복합 중재 (complex intervention)는 각각 1편씩으로 8.3%를 차 지하였다(Table 2). 각 논문의 중재에 대한 정보는 Table 3에서 제시된 논문 번호를 통하여 Table 8에서 확인 가능하다.
| Types | Article no. | Frequency |
|---|---|---|
| Self-management program | 2, 3, 6, 7, 8, 9 | 6 (50.0) |
| Exercise program | 4, 12 | 2 (16.7) |
| Client-centered approach | 5, 11 | 2 (16.7) |
| Intervention using digital device | 10 | 1 (8.3) |
| Complex intervention | 1 | 1 (8.3) |
| Total | 12 (100.0) | |
| Environments | Frequency |
|---|---|
| Community | 10 (83.4) |
| Hospital | 1 (8.3) |
| Both community and hospital | 1 (8.3) |
| Total | 12(100.0) |
2)중재가 적용된 환경
중재가 적용된 환경을 분석해 보았을 때 지역사회에서 중재를 적용한 논문이 10편으로 83.4%를 차지하였으 며, 병원 환경에서 적용한 논문과 지역사회, 병원 환경 두 군데에서 모두 적용한 논문이 각각 1편으로 8.3%씩 차지하였다(Table 3).
3)중재의 대상 클라이언트
중재를 적용한 대상을 분석해 보았을 때 뇌졸중 환자 를 대상으로 한 연구가 5편으로 41.7%였으며, 복합 만 성 질환을 대상으로 한 연구가 2편으로 16.7%를 차지하 였다. 그 외에 근위축증, 관절염, 다발성 경화증, 시력저 하 노인, 외상성 뇌손상 환자를 대상으로 한 연구는 각각 1편씩으로 8.3%씩을 차지하였다(Table 4).
| Classification of disease | Frequency |
|---|---|
| Stroke | 5 (41.7) |
| Multiple chronic conditions | 2 (16.7) |
| Amyotrophy | 1 (8.3) |
| Arthritis | 1 (8.3) |
| Multiple Sclerosis (MS) | 1 (8.3) |
| Older adults with Age-Related Vision Loss (ARVL) | 1 (8.3) |
| Traumatic Brain Injury (TBI) | 1 (8.3) |
| Total | 12 (100.0) |
3.참여를 평가하기 위해 사용된 평가도구
본 연구에서 분석한 총 12편의 논문에서 한 편의 논문 만 참여를 평가하기 위해 두 가지의 평가도구를 사용하 였으며, 나머지 11편의 논문은 각각 한 가지의 평가도구 를 사용하였다. Frenchay Activities Index (FAI), Reintegration to Normal Living Inex (RNLI)과 Stroke Impact Scale (SIS)의 ‘사회참여 (Social participation)’ 항목을 사용한 논문이 각각 2편으로 15.4%를 차지하였다. 나머지 평가도구들을 사용한 논문 은 각각 1편씩으로 7.7%를 차지하였다(Table 5).
| Applied measurement tools for participation | Frequency |
|---|---|
| Frenchay Activities Index (FAI) | 2 (15.4) |
| Reintegraton to Normal Living Index (RNLI) | 2 (15.4) |
| Stroke Impact Scale (SIS) -‘social participation’domain | 2 (15.4) |
| Activity Card Sort (ACS) | 1 (7.7) |
| Craig Handicap Assessment and Rating Technique-Revised (CHART-R) | 1 (7.7) |
| Canadian Occupational Performance Measure (COPM) | 1 (7.7) |
| Impact Participation and Autonomy (IPA) | 1 (7.7) |
| Occupational Gaps Questionnaire (OGQ) | 1 (7.7) |
| Physical Activity Scale for Individuals with Physical Disabilities (PASIPD) | 1 (7.7) |
| Social/ Role Limitation Scale | 1 (7.7) |
| Total | 13 (100.0) |
4.참여와 동시에 측정된 종속변인
본 연구에서는 참여와 동시에 측정된 종속변인 중 두 개 이상의 논문에서 참여와 동시에 평가된 경우를 표시 하여 Table 6에 제시하였다. 참여와 동시에 측정된 종속 변인 중 빈도수가 가장 높은 것은 ‘삶의 질’로 5개의 논문 에서 참여와 동시에 측정되었다. 또한, 감정 상태(우울, 불안)와 자기 효능감은 각각 4개의 논문에서 종속변인으 로 측정되었다. 일상생활동작에서의 기능적 독립과 작업 수행은 각각 3개의 논문에서 측정된 것으로 나타났다 (Table 6). 각 연구의 종속변인은 Appendix 1에서 확인 이 가능하다.
| Variables measured with the participation | Frequency |
|---|---|
| Quality of life | 5 (26.3) |
| Emotional status (depression, anxiety) | 4 (21.1) |
| Self efficacy | 4 (21.1) |
| Functional independence in ADL | 3 (15.8) |
| Occupational performance | 3 (15.8) |
| Total | 19 (100.0) |
Ⅳ고 찰
본 연구는 클라이언트의 참여 향상을 위한 중재에 대 하여 체계적 고찰을 시행함으로써 국내 작업치료사들에 게 클라이언트의 참여 향상을 위해 제공해야 할 작업치 료 서비스의 근거를 제공하고자 하였다. 본 연구에서 분 석의 대상이 된 논문은 총 12편으로, 질적 수준 및 동향, 중재와 관련된 요소, 참여를 평가하기 위한 평가도구, 그 리고 참여와 동시에 측정된 종속변인을 분석하였다.
본 연구에서 참여 향상을 위한 중재를 적용한 논문을 분석한 결과, RCT 논문이 전체의 58.3%였으며, 단일 그 룹 실험 설계가 전체의 41.7%로 근거의 질적 수준이 가장 높은 RCT 논문이 더 많은 비중을 차지하였다. 총 검색 년도를 반분하여 년도 별 연구 경향의 변화를 살펴보았을 때 논문의 질적 수준이 높아졌을 뿐만 아니라 논문의 편수 역시 증가하였다. 이러한 경향은 ICF가 발간된 이후 ‘참 여’의 중요성이 강조되고 있으며, 근래에 재활의 주된 목 적이 참여의 증진이 되어가고 있다는 보고와도 일맥상통 한다([Christiansen et al., 2005]; [Hildebrand et al., 2012]). [Law (2002)]는 작업치료사가 장애인 혹은 비장 애인의 참여를 증진시키고 만족시키는 데에 기여하기 위 해 특화된 직업이라고 하였다. 이러한 보고들을 토대로 분석한 본 연구의 결과는 작업치료 분야에서 점점 참여 증진에 대한 관심이 증가하고 있으며 수준 높은 근거 마련 을 위해 많은 연구가 진행되고 있음을 시사한다.
하지만 2008년에 Korner-Bitensky, Desrosiers와 Rochette가 세계적으로 진행한 뇌졸중 환자의 참여와 관련된 작업치료사들의 치료에 대한 조사에서는 아직까 지 50.0% 이하의 치료사만이 참여를 위해 중재를 시행 하고 있으며, 뇌졸중 환자의 성공적인 지역사회 재통합 과 참여를 위해서 이론적으로 어떤 측면을 보강해야 하 는 지와 연구 당시 작업치료에서 어떤 치료가 주를 이루 는지에 대한 차이가 크게 존재한다고 보고하였다. 따라 서 본 연구의 결과와 함께 추후 연구에서 현재 작업치료 사들이 클라이언트의 참여를 위해 실제 어떤 치료를 시 행하고 있는지에 대한 연구가 함께 진행된다면 연구를 토대로 한 치료의 이상과 실제 임상에서의 치료의 차이 를 줄일 수 있는 근거가 마련될 수 있을 것이다.
중재는 중재 방법의 종류, 중재가 적용된 환경, 대상 클라이언트로 나누어 분석을 진행하였다. 먼저 중재 방 법은 논문에서 제시한 용어에 따라 크게 다섯 가지로 분 류해 제시하였는데, 자기관리 프로그램(self-management program)이 가장 많았다. 중재들은 대부분 지역사회 중 심으로 제공되는 것으로 나타났으며, 40.0% 이상이 만 성 뇌졸중 환자를 대상으로 한 중재였다. 만성 뇌졸중 이 외에도 복합 만성 질환, 근위축증, 관절염, 다발성 경화 증, 시력저하 노인, 외상성 뇌손상 환자를 대상으로 하는 등 대부분 장기간 중재가 필요한 만성 질환을 대상으로 하였다. 실제로 [Lorig와 Holman (2003)]은 자기 관리는 만성 질환 환자들에게는 평생의 작업이며, 자기 관리 중 재는 질병의 기간에 걸쳐 일상적 관리에 대한 책임을 본 인이 져야 하는 만성 질환 환자들에게는 특히 중요하다 고 보고하였다. 또한 [Barlow, Wright, Sheasby, Turner와 Hainsworth (2002)] 역시 자기관리 프로그램 은 만성 질환자들에게 제공되는 다른 인지-행동적 중재 보다 더 좋은 효과가 나타난다고 보고하며 본 연구의 연 구 결과에 대한 근거를 제공하고 있다.
[Mukherjee, Levin과 Heller (2006)]은 뇌졸중 환자 에게 있어서 신체적 인지적 손상으로 인한 의사소통의 어려움은 사회적 접촉이나 사회적 고립으로 이어지며, 이는 뇌졸중 환자에게 보통 후유증을 불러오게 된다고 보고하였다. 이에 따라 약 30.0% 이상의 뇌졸중 환자는 급성기 상태에서 벗어나 병원을 퇴원하면 재활서비스나 장기간의 케어가 필요하며, 지속적인 지역사회의 지지가 필요하다([Centers for disease control and prevention, 2007]; [Chau et al., 2009]). 작업치료의 목적은 신체적 회복과 ADL에의 도움 이외에 심리사회적 증상을 최소화 하고 가족과 지역사회 속으로 환자들을 재통합시키는 데 에 있다([Chau et al., 2009]). 이와 더불어 본 연구의 결 과에서 지역사회 중심으로 뇌졸중 환자에게 많은 중재가 이루어진 것은 환자들로 하여금 지역사회에서의 통합을 위해 사회적 지지를 만들어주기 위함으로 사료된다.
참여를 평가하기 위해 사용된 평가도구로는 FAI, RNLI, SIS의 ‘사회참여 (social participation)’ 항목이 각각 2개의 논문에서 사용되어 15.4%씩을 차지하였다. 이러한 결과는 [Kim, cho와 lee 등 (2014)]의 연구에서 Activities Card Sort (ACS)가 3개의 논문에서 사용되 어 가장 많은 빈도를 차지한 것과는 상이하다. 이러한 결 과가 나온 이유는, 참여를 평가하는 연구의 설계는 ‘조사 연구’가 가장 많은 것으로 나타났으나 참여 향상을 위한 중재를 확인하는 것이 목적인 본 연구에서는 조사연구를 모두 제외하였으며, 조사 연구에서 사용되는 평가도구와 중재 효과를 확인하기 위한 평가도구의 유형이 다르기 때문인 것으로 사료된다. 추후에 조사 연구에서 사용되 는 참여 평가도구와 중재의 효과를 확인하기 위한 평가 도구를 구분하여 분석하는 연구가 필요할 것이다. 또한 사용된 평가도구의 빈도수에 많은 차이를 나타내지 않았 는데 이는 중재의 효과를 확인하기 위하여 특별히 많이 사용되는 평가도구가 없으며, 참여를 평가하고자 하는 연구자들이 연구 형태와 측정하고자 하는 참여의 방향에 따라서 도구를 선택하기 때문인 것으로 사료된다. 이에 따라 중재 결과 분석을 위해 참여를 평가하는 데에 민감 성이 높으면서도 ICF에서 제시하는 참여의 9가지 카테 고리를 모두 담을 수 있는 평가도구를 개발하는 것 역시 고려하여야 할 것이다.
본 연구에서는 참여와 동시에 측정된 종속변인을 살펴 보았는데 참여와 동시에 측정된 종속 변인 중 빈도수가 가장 높은 것은 ‘삶의 질’로 5개의 논문에서 참여와 동시 에 측정되었다. 그 다음으로는 감정 상태(우울, 불안)와 자기 효능감, 일상생활동작에서의 기능적 독립 및 작업수 행 순으로 높은 빈도를 나타냈다. 각 논문에서는 종속변인 들 간의 관계를 밝히고 있지 않지만 [Chau 등 (2009)]의 논문에서는 우울이 참여 제한에 영향을 주는 직접적 요소 라는 것이 확인 되었다. 추후에는 우울뿐만이 아니라 본 연구에서 제시된 종속변인 간에 어떤 관계가 있는지를 확 인하여 중재 시에 효과적으로 참여의 수준을 향상시킬 수 있는 방법의 근거를 제시해야 할 것이다.
본 연구는 분석 대상에서 국내 연구와 사례 연구를 제 외하였기 때문에 모든 중재 방법을 포함하였다고 할 수 없으므로 분명한 제한점이 존재하며 추후에는 모든 중재 를 포함할 수 있는 설계를 따라야 할 것이다. 하지만 본 연구는 선행연구와 비교하였을 때 분명한 임상적 의의가 존재한다. 선행연구에서는 특정 대상군과 특정 중재 방 법, 참여 평가도구를 중심으로 체계적 고찰이 이루어진 반면 본 연구와 같이 참여 향상을 위한 중재에 관한 종합 적인 고찰은 이루어지지 않았다. 때문에 본 연구는 전반 적인 고찰을 통한 결과를 토대로 실제 현장에서 참여 향 상을 목적으로 이루어지는 작업치료 중재에 근거를 제공 하고자 한 데에 의의가 있다. 실제로 [Berger 등(2013)] 의 연구에서는 저시력 노인들을 위한 참여 향상 중재를 수집하여 체계적 고찰을 시행하였으나 문제 해결 접근, 복합 서비스, 기술 훈련, 재가 방문 및 환경 수정의 네 가지 중재 방법에 대한 결과를 통해 중재의 근거 수준만 을 소개하였다. [Yu 등 (2014)]의 연구에서 역시 다발성 경화증 환자의 참여 향상을 위한 세 가지 중재법과 각 연 구의 결과를 통한 근거 수준만을 소개하였다. 이외에도 [Magasi와 Post (2010)]와 [Perenboom과 Chorus (2003)]는 각각의 평가도구들이 ICF의 기준에 얼마나 부 합하는지를 체계적 고찰을 통하여 소개하였으나 각각의 평가도구들이 어떠한 연구에서 어떻게 사용되는지에 대 한 논의는 이루어지지 않았다.
앞으로 이루어지는 참여 관련 연구에서는 앞서 언급한 바와 같이 작업치료사들이 클라이언트의 참여를 위해 어 떤 실행을 시행하고 있는지에 대한 연구, 민감성이 높으 면서도 ICF에서 제시하는 참여의 9가지 카테고리를 모 두 담을 수 있는 평가도구의 개발, 참여와 동시에 주로 측정되는 종속변인 간에 어떤 관계가 있는지를 확인하는 연구 등을 시행하여 중재 시에 효과적으로 참여의 수준 을 향상시킬 수 있도록 그 근거를 제공하고, 연구에서 언 급하는 이상적인 참여 향상 중재와 실제 작업치료 현장 에서 실행되는 중재와의 차이를 줄일 수 있도록 연구의 방향이 발전해 나아가야 할 것이다.
Ⅴ결 론
본 연구는 클라이언트의 참여 향상을 위하여 어떠한 작업치료 중재를 사용하고 있으며, 중재와 관련된 정보 가 나타내는 경향을 알아보기 위하여 총 12편의 논문을 중심으로 체계적 고찰을 실시하였다. 참여 향상을 위한 작업치료 중재를 주제로 한 논문의 질과 양은 계속해서 늘어나고 있는 추세였으며, 중재로는 자기관리 프로그램 이 가장 많은 빈도를 보였다. 이러한 중재는 대부분 지역 사회에서 만성질환 환자들에게 실행되는 것으로 나타났 다. 하지만 아직까지 참여 향상을 평가하기 위해 일률적 으로 사용하는 평가도구는 없었으며, 국내에서 참여와 관련된 종속변인간의 관계를 확인한 연구는 없었다. 따 라서 추후에는 참여 향상을 평가할 수 있는 타당도 높은 평가도구를 개발하고 종속변인 간 관계를 확인하는 연구 가 필요할 것이다. 본 연구는 종합적인 정보의 고찰을 통 하여 작업치료 임상 현장에서 적용할 수 있는 참여 향상 을 위한 작업치료 중재 및 관련 자료를 제시하는 기초자 료가 될 것이다.
References
Appendix 1.
| No. | Author (yr) | Participants | Intervention | Intervention intensity/ duration | Dependent variables | Measurement for participation | Results |
|---|---|---|---|---|---|---|---|
| 1 | [Mayo et al. (2015)] |
93 people with chronic stroke living in the community |
Rest of Your Life: Mission Possible© program - Complex intervention - included exercise and project-based activities promoting learning, leisure, and social activities |
12 mo 2 sessions / week 3 hr/ session |
Related participation |
Reintegration to Normal Living Inex (RNLI) |
Significant change on the RNLI at all time points statistically significant increases in all study outcomes on average over all persons |
|
Participation outcome | |||||||
| Others | |||||||
|
Hours spent in meaningful activity Gait speed Depression Apathy Sroke-specific HRQL Health rating HRQL | |||||||
| 2 | [Garvey, Connolly, Boland, & Smith (2015)] |
26 participants with mmultimorbidit y in the community care areas |
Occupational Therapy Led Self-Management Support Program (OPTIMAL) -Weekly group meeting -Occupational therapy focus -Peer support -Goal setting and self-management |
6 weeks 1 session / week |
Related participation |
Frenchay Activities Index (FAI) |
Improvement in frequency of activity participation (FAI) for the intervention group was significant compared to the control group Significant improvements in perceptions of activity performance, satisfaction, self-efficacy, independence in daily activities and QoL No significant differences among the control and intervention group in anxiety, depression, self-management scores or healthcare utilisation |
|
Frequency activity participation | |||||||
| Others | |||||||
|
Satisfaction with and ability to perform activities Independence in ADL Anxiety and depression Self-efficacy HRQL Self-management support HCU | |||||||
| 3 | [Rietber g, van Wegen, Eyssen, Kwakke l, & MS study group (2014)] |
21 people with Multiple Sclerosis in community outpatient clinic |
Multidisciplinary Outpatient Rehabilitation (MDR) programme - OT, PT, SW |
PT - 12 weeks - 1 session /week - 45 min /session OT, SW - as-needed 1 hr/session |
Related participation |
Impact Participation and Autonomy (IPA) |
No significant within-group effect in both groups about the all outcome measures from baseline to 12 or 24 weeks |
|
Participation and autonomy | |||||||
| Others | |||||||
|
Related fatigue Impact of Multiple Sclerosis (MS) Functional independence | |||||||
| 4 | [Kim, Cho, & Lee (2014)] |
13 chronic stroke patients in the community |
PT, OT Community Walking Training Program (CWTP) -within the real environment (near hostpital setting, outside of the hospital setting on uneven ground, outside of the hospital setting on uneven ground with obstacles, shopping center) |
PT + OT - 60 min - 5 sessions /week - 4 weeks CWTP - 4 weeks - 5 sessions /week - 30 min /sesseion |
Related participation |
Stroke Impact Scale (SIS) -‘social participatio n’domain |
Significant improvements in social participation and walking function after the intervention, Significantly greater improvement than the control group in social participation and walking function in CWTP group |
|
Social participation | |||||||
| Others | |||||||
|
Walking function | |||||||
| 5 | [Bertilss on et al. (2014)] |
129 people both inpatient and outpatient with stroke |
Client-centered activities of daily living (CADL) intervention -9 steps (identified 3 goals for activities he/she wanted by COPM and learn problem-solving strategy etc.) |
non | Related participation |
SIS -‘social participatio n’domain |
No difference between groups in the primary outcome (fatigue), and participation significantly No difference between the CADL and the UADL groups in the SIS’s domain‘participation |
|
Perceived participation | |||||||
| Others | |||||||
|
Independence in ADL Life satisfaction Home- help service and satisfaction with training | |||||||
| 6 | [Toole, Connoll y, & Smith (2013)] |
16 Community living Individuals with multiple chronic conditions |
Occupationl-based self-management progrmme -Educational and Individual goal-setting component |
6 weeks 1 seesion /week |
Related participation | FAI |
Significant differences in post-intervention’s and 8-week follow-up’s participation, self-perceptions of occupational performance and satisfaction |
|
Participation in occupations | |||||||
| Others | |||||||
|
Occupation performance Self-efficacy Depression and Anxiety Quality of life | |||||||
| 7 | [IJspeert et al. (2013)] |
8 patients with subacute neuralgic amyotrophy in outpatient clinic |
Multidisciplinary intervention program -Support patients in their self-management strategies |
Each therapy (OT, PT) for 8 hr spread over a 16-week period |
Related participation |
Canadian Occupational Perforamanc e Measure (COPM) |
Statistically significant improvements in COPM and Shoulder Rating Questionnaire (SRQ, measurement for activities and function) scores |
|
Participation | |||||||
| Others | |||||||
|
Body function Activities and function Quality of life Personal factor | |||||||
| 8 | [Bethea, Lovett, Cooks, & Bell (2010)] |
10 clients living with arthritis in the local community center |
Self-Help Program -Understanding pains -A self-management plan -Hints, tips, gadgets, and resources -Keeping body healthy -Solving problems -Medical resources |
6 weeks 1 sessions /week 2 hr/ session |
Related participation |
Social/ role limitation scale |
Based on participants’ responses, increased levels of participation in social activities and expansion of social roles following the program implementation were evident |
|
Social roles, participation | |||||||
| Others | |||||||
|
Self-efficacy behaviors Energy and level of fatigue | |||||||
| 9 | [Packer, Girdler, Boldy ,Dhaliwa l, & Crowley (2009)] |
12 older adults with age-related vision loss (ARVL) in the nursing home |
Vision Self-Management (VSM) progrmme - Understanding VL - Making the most of your vision and other senses - Staying in touch - Looking & feeling right - Managing at home - Stepping out - It’s time for fun - Living in the community and graduation |
8 weeks 1 session /week |
Related participation |
Activity Card Sort (ACS) |
Statistically significant increases in participation, measured by the ACS at post-test Statistically significant results in both general health and vision specific domains |
|
Participation in life situation | |||||||
| Others | |||||||
|
Emotional status Quality of life Adaptation ARVL self-efficacy | |||||||
| 10 | [Gentry, Wallace, Kvarfor dt, & Lynch (2008)] |
23 communitydwelling Severe Traumatic Brain Injury |
Personal digital assistants (PDAs) as cognitive aids PDA Training (facilitation as participants learned to use th PDA to assist in performing everyday life tasks.) Post-training period (trouble-shooting questions by teledevice) |
8 week (post-training period) |
Related participation |
Craig Handicap Assessment and Rating Technique-R evised (CHART-R) |
Statistically significant results between pre and post training subscores were found in CHART-R(domains‘independenc e, cognitive, mobility, and occupation’) Improvement was noted significantly for Self-ratings of participation, occupational performance and satisfaction with occupational performance |
|
Participation in everyday life tasks | |||||||
| Others | |||||||
|
Occupational performance and satisfaction | |||||||
| 11 | [Egan, Kessler, Laporte, Metcalf e, & Carter (2007)] |
6 chronic stroke survivors discharged to a non institutional setting (community) |
Client-centered occupation-based approach guided by COPM, OPPM - coaching, education, changes to the physical environment, use of sources with the goal of enabling the client to achieve identified goals |
8 visits over 2~4 mo |
Related participation |
RNLI |
No differences between the intervention and control groups at posttest on the RNLI score Statistically and clinically significant difference in only satisfaction with performance between intervention group and control group |
|
Participation | |||||||
| Others | |||||||
|
Occupational performance Satisfaction with current level of functioning Well-being | |||||||
| 12 | [Pang, Eng, Dawson, McKay, & Harris (2005)] |
32 older adults with chronic stroke in the community |
Exercise program Fitness and Mobility Exercise (FAME) program - Cardiorespiratory fitness and mobility - Mobility and balance - Leg muscle strength Hip protector |
Exercise program - 19 weeks - 3 session /week - 1hr/session FAME program - 10 min initially, with increment of 5 min every week |
Related participation |
Physical Activity Scale for Individuals with Physical Disabilities (PASIPD) |
More improvement in Intervention group at PASIPD scores than the control group No significant differences between groups in PASIPD Significantly more gains in Cardiorespiratory fitness, Mobility, Leg muscle strength than control group |
|
Activity and participation | |||||||
| Others | |||||||
|
Cardiorespiratory fitness Mobility Leg muscle strength Balance Bone mineral density Respiratory exchage ratio |